





Medical Robots: Who’s Really Holding the Knife?
By Farrukh Anique ||
“I would never trust an AI-driven car to drive me anywhere. It is like putting my life in the hands of a machine,” a friend told me recently. Interestingly, he is a medical robotics researcher, busy designing a robot that slips a needle into the spinal canal to deliver pain-relieving drugs. Ironic, is it not?
So, when we agree to a medical or surgical procedure done with robotic assistance, are we really handing our lives over to machines? How safe are these steel “hands” we invite so close to our bodies? Let us look beneath the smooth plastic covers to see how medical robots actually work and how they are designed to protect the very lives they seem to threaten.
When someone says “robot,” most of us picture the same thing: a metal human with two arms, two legs, a pair of shiny eyes, maybe even a friendly, or slightly creepy, face. But that cartoon in our heads is almost never what real robots look like. Surgical robots are, in essence, sophisticated tools that try to imitate the precision of human hands during an operation. They do not need faces or fingers to do that. If you walk through a hospital, most of the devices you see will just look like machines: boxes, arms, cables, screens.
That is exactly what my friend meant when he said he could not trust his life to “a machine.” But when you are lying on an operating table and a robotic system is working a few centimeters under your skin, you are not truly trusting the machine. You are trusting the person behind it – the surgeon at the console, who sees your organs magnified on a screen and directs every tiny movement. Medical robots do not decide what treatment you receive, and they do not write the plan for your surgery. They simply carry out the strategy your doctors have already designed after thinking, debating, and worrying over your case in a very human way.
Every medical robot is built from a handful of basic parts, and it makes sense to start with the one that matters the most to the patient and to the designers as well. Engineers call it the “end effector,” but you can think of it as the robot’s hand, the part that actually touches the body. This hand can take many forms. In one procedure it might be a fine needle, in another a tiny scalpel, in another a delicate gripper with small jaws. Depending on the surgery, the end effector may cut and dissect, place stitches, take a biopsy sample, inject or remove fluids, steer catheters and guidewires through blood vessels, or hold an ultrasound probe in just the right position on your stomach. All the motors, sensors, and software exist for one purpose: to guide this small, specialized tool so it can do its job with as much precision and as little damage as possible.
During surgical procedures, surgeons usually control the motion of the end effector with a primary device, often called the “master controller.” It might look like a joystick, a pen, or a small pistol-shaped handle dotted with buttons. The surgeon’s hands stay on this master controller, making calm, deliberate movements, and the end effector (the slave side) quietly follows. But it is not a simple one-to-one copy. Between master and slave, the motion is cleaned and refined: Tiny hand tremors and sudden jerks are filtered out, movements are scaled down so a big sweep of the hand becomes a tiny shift at the instrument tip, invisible boundaries and pivot points are enforced so the tool pivots safely at the entry point, and both force and speed are carefully controlled. In other words, the robot does not make the surgeon superhuman, it simply helps their human hands behave at their very best where it matters most.
To truly see what they are doing, surgeons need more than steady hands, they need good eyes, and in modern operating rooms, those eyes are electronic. An imaging device, such as a camera, CT scanner, ultrasound probe, or MRI, feeds pictures to a monitor, giving the surgeon a window into the body. Before those images appear on the screen, they are often processed and enhanced: Contrast is adjusted, noise is reduced, and important structures are made clearer.
Today’s imaging systems can even blend different types of images and use image processing techniques to highlight suspicious areas, such as potential cancer nodules. On the screen, the surgeon can mark target regions directly, sketch possible paths, and plan safe trajectories with a precision that would be impossible by touch and intuition alone. In a sense, the imaging system turns the patient’s hidden anatomy into a map that the surgeon and the robot can read together.
Every active robot needs a way to move, and that job belongs to its “actuators,” the muscles of the robot. These may be electric motors, fluid-powered actuators, smart flexible materials, or other clever mechanisms. They draw energy from one of various kinds of sources and turn it into exactly the kind of mechanical motion the task demands. Modern actuators can be astonishingly precise, delivering tiny, smooth movements deep inside the body – motions so controlled and delicate that no human hand, however skilled, could ever quite match them.
As the robot works, the surgeon must stay aware of what is happening inside the patient, inside the machine, and right at that fragile contact point between metal and tissue. That is where sensors step in. They are the eyes and ears of the robot, and in a way, borrowed senses for the surgeon. They reach beyond the limits of human sight and touch, streaming back information no naked eye or fingertip could ever provide.
Sensors track the position and motion of tools and tissues, and they measure the forces and torques where they meet. Others watch over the robot’s own health, monitoring temperature, current, and pressure, while cameras and other imaging sensors capture pictures and video for processing and presentation. Together, they allow the system to regulate the robot’s performance and the team to monitor the patient’s condition at the same time.
Then comes another crucial component: the control system. This is the software, the brain of the robot. Inside it lives the code for everything the robot is designed to do, from how it should perform its tasks to how it should react if something unexpected goes wrong. It talks to the actuators, listens to the sensors, and makes sure the robot moves exactly as it is supposed to.
The control system also draws the safety boundaries and refuses to cross them. Even if a human makes an error in judgment or pushes the controls in the wrong direction, the software can step in, limit the motion, and prevent the robot from doing something that could harm the patient.
When you put all of this together, the picture becomes much clearer. The end effector may be the part that touches your body, but it does so only under the watchful eyes of sensors, the steady muscles of actuators, and the strict rules of the control system. Behind them stand engineers who test every line of code, doctors who refine procedures, and regulators who demand proof that the whole system behaves safely, even when something unexpected happens. Patient safety is not left to a single clever gadget, it is built up in layers, from mechanics to electronics to software to the careful people who design, test, and use these machines.
So, who is really holding the knife in a robot-assisted surgery? In a narrow sense, it is a steel instrument guided by motors and algorithms. In a deeper sense, it is still the surgeon, supported by a quiet crowd of sensors, actuators, control systems, and unseen researchers who have spent countless days and nights making sure that every motion is as safe and effective as possible. The robot is not there to replace human care but to give careful hands better tools. As patients, we are not trusting our lives to a cold machine running on ones and zeros; we are trusting a very human team that has chosen to work through these ones and zeros in order to harm less, see more, and heal better.
The Author
Farrukh Anique is a PhD student immersed in mechanical engineering at Chonnam National University. Originally from Pakistan, he’s not all about gears and equations though. He’s got a real love for the performing arts, culture, literature, and languages. He is an amateur theater actor, a short-story writer, and he speaks five languages. In his spare time, he dives into Korean culture and history, soaking up the vibrant traditions and stories that spark his curiosity. Oh, and he absolutely loves strawberries.
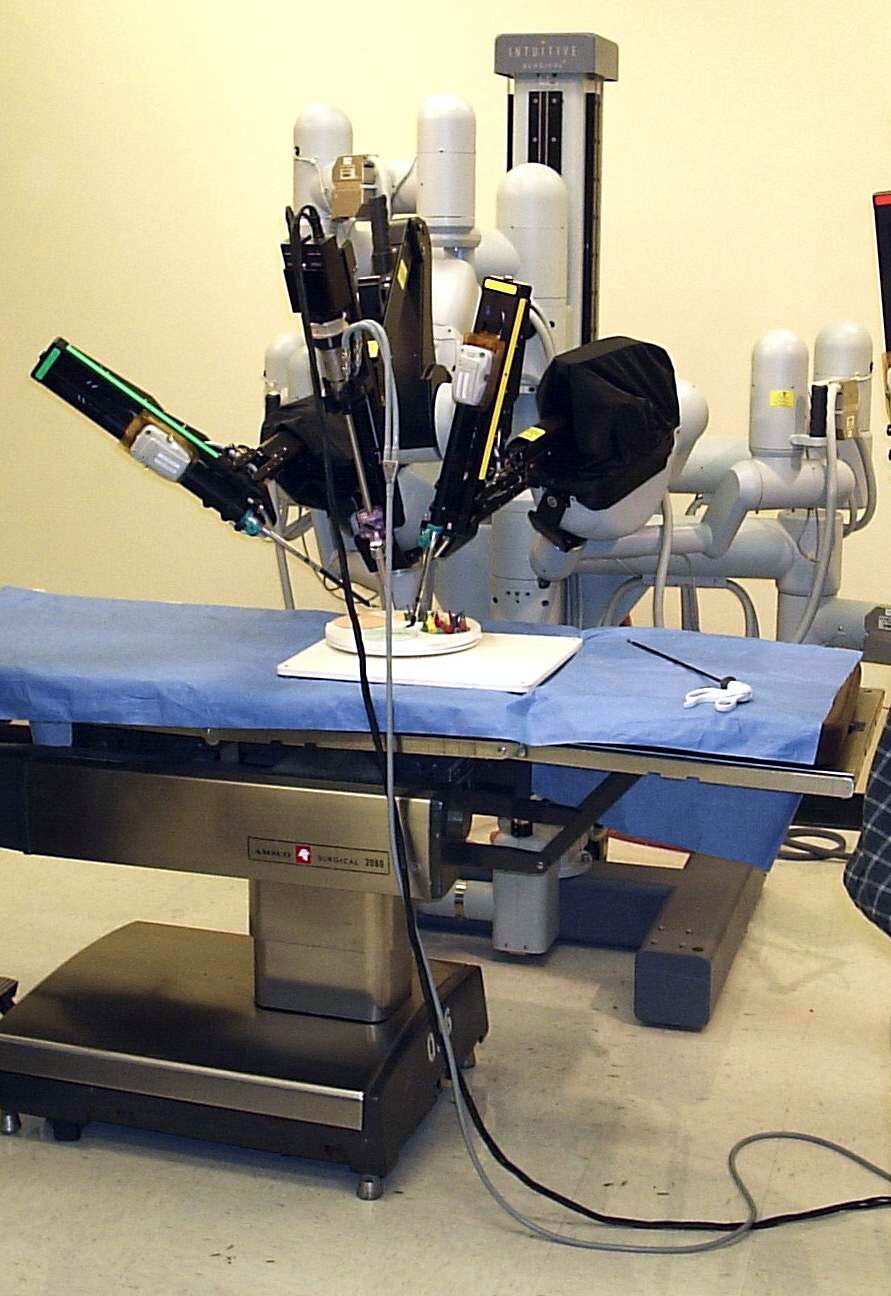
Cover Photo: Robotic surgical system. (Tatyana Makarova on Vecteezy.com)